All of our in-person Houston area and Zoom meetings are canceled this Thanksgiving Thursday. Meetings will resume next week.
Recovery Articles
Tonight’s Sugar Land Meetings Canceled
Our host church will be closed tonight so we will not be meeting. Please join our Zoom meeting. Contact info@castimonia.org for Zoom meeting links.
John Piper: Sexual Sin In Ministry
originally posted February 27, 2013
Wisdom from the heart of a true father!
rgh
“For the last twenty years thousands of men from across America struggling with sexual sin have come to our intensive counseling workshop. Over half were pastors and missionaries.
I wish our experience was unique.
Several years ago a seminary professor told me: “We no longer ask our entering students if they are struggling with pornography, we assume every student is struggling. The question we ask: ‘How serious is the struggle?’”
One missions agency told me that 80% of their applicants voluntarily indicate a struggle with pornography, resulting in staff shortages on the field.
Pornography is just one level of sin, a form of visual sex, or heart adultery. Physical adultery includes an affair, multiple affairs, prostitution, and homosexuality. Other sexual behaviors within the ministry are such heinous “unfruitful works of darkness . . . it is shameful even to speak of the things that they do in secret” (Ephesians 5:11–12).
To face the crisis we must correctly understand the nature of the problem, ask God to search our own hearts, and be committed to restore each one caught in sexual sin “in a spirit of gentleness” (Galatians 6:1).”
The Evolution of Revolution: Understanding Sex Addiction
Originally posted February 25, 2013
Patrick Carnes: Evolution of Revolution, Understanding Sex Addiction
http://www.counselormagazine.com/detailpage.aspx?pageid=1443&LangType=1033&id=6442451121

It was a cold late fall evening, and I was about to give my first address to the medical staff of Golden Valley Health Center. This facility was an 850-bed hospital located in suburban Minneapolis. It had a long and respected tradition as a psychiatric facility that also treated substance abuse. The year was 1984 and Out of the Shadows had appeared in January. While the reception that year certainly started controversies, there was also real and substantive support in both the professional and the recovering communities. The very first inpatient program for sex addiction was set to open in January 1985.
My job that night was to be the keynote speaker for the annual medical staff dinner for close to 300 doctors, clinicians and their spouses. My purpose was to underline the importance of this new sex addiction program. I was nervous, but I strategized that what had worked best for me was to use compelling cases to paint a picture of real need. One example was that I had a letter from the wife of a physician who had joined Sex Addicts Anonymous (SAA) and received treatment. It was a moving tribute to the power of treatment and her gratitude for the help received. Also I knew I had spouses in the audience as well as doctors, so it was a way for all to identify. And the author had kindly given me permission to share her sentiments anonymously. So I was ready.
Yet I was totally unprepared for what happened. After the lovely supper had been served and eaten, the hospital administrator went to the podium and started his introduction for my talk. It was a cue for a staged walkout. Suddenly about half of the audience simply got up and left. They were led by the most significant psychiatric group on the medical staff. Even more stunning was that key members of the administration staff joined the exodus in protest to the hospital opening a sex addiction program.
Over my career I have had critics, hecklers and reluctant staff members. But that moment was a defining moment in which I and what I represented were clearly not welcome. I remember the spotlights being on me, and everyone waiting for what I would say. I stood there, notes and letter in hand, transfixed with the fear that I had no right to be there. I wondered if I should walk away, but then I looked at that letter and knew I needed to speak the truth I knew. So I stepped forward and with a somewhat halting voice thanked those who had stayed and told them why I was there.
At the time Golden Valley was owned by Compcare Corporation and its president was Dr. Richard Santoni. He and I had spent afternoons together reviewing data and cases about sex addiction. His resolve pushed all of us to opening that program on time. Once open, a transformation occurred. The patients were profoundly grateful to have a place that understood their problem. Compared to most patients in the facility, they were not only hurting but also motivated. Soon the Sexual Dependency Units became the place where everyone wanted to work. Even the physicians who had walked out during my address changed their minds. When the patients came, the legitimacy of the problem was clearly established. The reputation for breaking new ground and being of genuine help compared to the revolving psychiatric doors characteristic of the day was more than attractive. Plus in 1985, physicians would be paid by patient as a separate bill. With $265 a day at stake, those who walked out the night of my talk now demanded to be put on the rotation list.
Then new institutional battle lines were drawn. The word spread that these were interesting, motivated patients who could afford to pay. Doctors wanted to be these new patients’ doctors but did not have time to go through the training to understand what the staff was asking of the patients in the program. Thus you had doctors giving well-meaning but ill-informed advice that was contrary to the precepts of the program. Clearly, a training program was necessary. Similarly, referents were asking for help because now that there was help, others followed locally from 12-step groups. Clinicians also saw the progress made in the hospital but questioned how to maintain momentum when the patient returned to the real world.
Other questions arose. With so many patients coming to the clinic, could they be put into groups? What was the criteria for inpatients other than desperation? Did treatment work for offenders? Were offenders part of a continuum, a separate problem or was there an overlap with sex addiction?
Leading the requests to join the new program were various directors of physician health programs. Most notable among those was Dr. Richard Irons, who eventually joined the staff at Golden Valley, and Dr. David Dodd from the Tennessee Medical Foundation, who worked hard to open the doors to understanding for those who treated physicians with addictions. Both of these men rose to the challenge of leadership and contributed dramatically to the knowledge and acceptance of sex addiction as a problem. Now physicians were joining in the fight and advocating for further knowledge.
The problem then was how to acquire that knowledge. I remember sitting at lunch with colleagues from Golden Valley in May of 1985.
We were celebrating all the progress being made and a recent television show with Oprah Winfrey, which brought over 11,000 calls to the hospital seeking help. We were talking of the new training necessary. Suddenly I experienced a deep fear within myself and I tuned my colleagues out. I realized we were celebrating the opening of the hospital program as an end goal that would solve the problem. Yet it was but a waypoint. All these unanswered questions existed. How would we find the answers and pay for the research? We had worked so hard just to get to the point where we had a facility. So many prejudices and professional barriers had to be overcome. We had just begun. When I tuned back to my friends, the tone of the lunch changed when I shared what I was thinking.
Still, throughout this whole journey people were ready to help. Money was found. A team of eight researchers, including myself, started to gather data. Hundreds of therapists opened their practices to this work. And just short of 1,000 sex addicts and many of their partners joined in the effort. The pooling of the efforts of all of us helped us to fashion training as a collecting point for the story of recovery that was emerging. It was the beginning of the Certified Sex Addiction Therapist program whose participants today we call CSATs. The resistance to our work did not stop, since there frequently were obstacles such as “that may work in the city but will not in the country” or even, “that will never work in my country.” Plus the process of discovery led to more questions and complications. Yet we persisted in pooling our knowledge.
What we have experienced is now a global phenomenon. For example, a young woman who just started working on her CSAT returned to a very rural part of Canada. She was told such clinical interventions would never work there and certainly not with families. But with the backing of her hospital she now directs a thriving sex addiction program with heavy family involvement. In Slovenia, a country of only two million, a family physician supports the beginning of a 12-step program for sex addicts. Today she has left family practice behind and devotes herself to helping families of sex addicts. In South Africa, I attended an SAA meeting of about 125. I was struck by the level of knowledge and good recovery in the room. I asked how this happened. It was business leaders who knew something had to be done who had bought materials and distributed them for free. And then they subsidized interested therapists who sought training.
One of the more interesting stories internationally is what the Norlien Foundation in Alberta, Canada, has been able to achieve. Once they became clear about the problem of addiction, they focused first on prevention. They created an initiative for early childhood education and family wellness that leveraged foundation and provincial funds into an amazing resource for Canadian families. Then they brought the very best science experts in addiction together for a series of conferences involving policymakers, government officials and healthcare professionals. They completely revamped the approach to talking about sex addiction by focusing on brain development and trauma. Then they ramped up the discussion into understanding addiction as a brain problem–of which sex was one of the options. They created an initiative to educate providers and physicians. They invited an American think tank called Frameworks to help with a cultural intervention.
(see Figures 1 and 2)
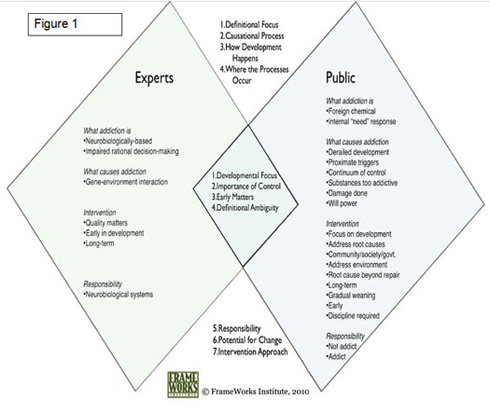
Figure 1
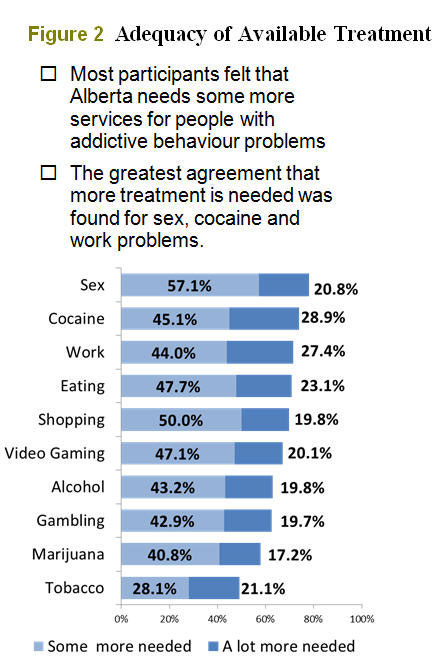
Figure 2
Their first effort was to show that a consensus existed amongst all the various professions involved. Amongst the average citizen, however, there were all kinds of perceptions, far from those of the research consensus, and few areas of agreement. Figure 1 graphically summarizes where the discontinuities were. The second initiative was a massive education effort of the public, which showed an astounding shift in understanding. Figure 2 lists what emerged in a survey of 4,000 citizens. Sexual compulsivity was at the top of the list. (For more information, please go to their website norlien.org. It is an open source treasure trove of useful information.
Clearly the time has come for a global conversation. Hosted by Caron and U.S. Journal Training, but supported by key professional associations and treatment facilities, the 1st International Conference on Sex & Love Addiction will be held April 4–6. A planning group was formed with clinicians and physicians from around the world. The conference is being held in Brooklyn, New York, an international city with easy access. The goal is to again share what we know across disciplines and countries.
Sex addiction does have uniqueness. It requires clinicians who understand addiction, sex therapy, family therapy, trauma, sex offending and brain science. Physicians need to step past traditional psychopathology and recognize process addictions. Cultural differences are a factor. We, for example, are the world leaders of pornography, producing over 400 million pages last year alone (the closest other country is Germany with 10 million pages). Yet the irony is that terrorists, including Osama bin Laden, were consumers of porn. In putting together this conference we were not surprised to learn that the pornography consumption among United States military personnel emerged as a significant issue and the United States military is not the only military struggling with this concern.
Sex addiction is most difficult to treat because of the intimacy and centrality of sex to being human. At a recent conference, an elderly clinician from China leaned over and whispered to me, “You do know this is the most important global issue we probably have. It is a huge problem in our country. But no one wants to talk about it.” She looked at me with tears in her eyes as she left. She did not even hear my whispered, “I know” as she now was already focused on her labored walking.
My seatmate on the plane was a professional man. After talking with him for a few minutes I was aware that the language he used was 12-step based. I asked if he was in the program and he said yes, that he had been in AA for four years. We talked some about it. Then he leaned over and asked me if I knew anything about sex addiction. I said that I had been in a program of sex addiction recovery for some time. He then said, “I have three sponsees who are struggling because they have not surrendered to their sex addiction. I finally said to one of them that I could not help him any longer if he did not do what his sex addiction treatment asked him to do, because he would die.” He then leaned over and asked me if that happens often. I nodded my assent. He leaned back and said, “We have to wake up.” I said, “I know.”
So consider this issue of Counselor a wake-up call. Sex addiction is not just a collateral problem to be referred on. We have invited some of the best providers in the country to share with you here some of the latest knowledge and tools. Rob Weiss is amazing at his ability to track how digitalization is transforming the key variable in addiction acquisition: availability. Suzanne O’Connor and Stefanie Carnes review some of the latest instrumentation available. Three private practitioners talk about what it has been like to build their practice around sex addiction. Two inpatient providers talk of revising their programs in light of evidence-based practice. Caron Foundation staff share what they learned when they systematically assessed clients for sex addiction. The Pine Grove staff at Gentle Path share their realization of how differentiated their patient population was when they simply tracked the patients as they withdrew from the program. As you read you will also learn how 12-step programs have provided so many good options across the world.
The professionals writing here are both evolutionary and revolutionary, doing what good medicine and science has always done. We make things better by pooling what we know and helping each other. Now our network will extend across the world. In the words of a song from the sixties, “There’s something happening here. . .”
I sold an old farm that my wife and I had while she was alive. In it all the research records were stored that we started collecting in 1985. Among them were all the stories of the 1,000 addicts and their partners. The average transcript was about 80 to a 100 pages long, single spaced. These stories were in addition to all the data collection we did, which took hours to fill out and seven years to collect and analyze. In moving my records, I sat on the floor, opened the boxes and was flooded by memories of all the people who had shared their pain, struggles and success. I heard their voices and wept. I whispered out loud, “I know.” And I think many more will know now too. Thank you.
My Dad Taught Me That My Sex Appeal Matters Most to Men
How fathers contribute to girls’ sexualization
Published on June 21, 2012 by Kerry Cohen in Loose Girl
My sister and I grew up as teenagers in our father’s home. We lived in a three-bedroom apartment in Fort Lee, New Jersey, right across the George Washington Bridge from Manhattan, and I often gazed out my bedroom window to the lights of that bridge, which made me believe that the world contained excitement, though what kind of excitement I didn’t yet know. When my friends came over, my father’s eyes scanned their bodies—these strange, beautiful creatures. Later, he would tell me he thought a friend was cute, that if he were in high school with us, he’d have a little crush. When he said things like this, my stomach hollowed out. I’d back away, eager to get back to the safety of my room. He had a girlfriend, and sometimes he grabbed her ass in front of me, or she rubbed his ear with her thumb in the car and he’d lean toward her, making a sexual noise I didn’t want to hear. He commented on females wherever we were. He’d check them out, eyeing their tight asses. He joked that he liked women who looked cheap, and though I rolled my eyes and laughed with him, I didn’t find it funny at all. Because what did it mean for me, a girl just past puberty, hoping to be wanted by the world? What would I have to do to get love and attention? Who would I have to be?
My sister’s and my bedrooms were at the end of a long hall, while my father’s room was right off the living room. He would often rush by the hallway, afraid, it seemed, to look our way. He had grown up with two brothers, and now here were two girls, as alien to him as boys were to me. I like to think now that he didn’t know the harm he did when he commented on those other women, on my friends. I like to think that just as he avoided that hallway, he avoided thinking too much about the things he said. And, meanwhile, the beliefs he had about women negatively affected his life. After my parents’ divorce he dated a string of women, mostly for the wrong reasons, (i.e., their looks). He looked past women who might have made better matches for him, and he held onto women with whom he had little connection. Other than being sexist in this way, my father was highly intelligent, deeply convicted in his liberal beliefs, creative, and terribly funny. His issues with women were the bane of most of his life.
While I was growing up, the culture was exploding with sexual images. Commercials showed half-naked women reeling in men. Clothing for young women was more suggestive than ever. Everywhere I looked, girls were taking off their clothes and grinding against men. Even the cheerleading team in my high school, which my father wanted me to join, performed risqué routines. Everywhere around me was sex. There was no escaping it, not at home, not on TV, not anywhere. And, let’s face it, my father didn’t escape it either. He’d grown up in the 1950s when men were seemingly afforded every last privilege, and then he divorced in the 1970s, during the sexual revolution.
Like most every woman I know, I grew up sexualized, which the American Psychological Association partially defines as believing one’s value is tied to her sex appeal and sex behavior, and allowing oneself to be sexually objectified and/or used. When I look back at my adolescence, I’m not sure I had a fighting chance against this. No one helped me build interests in anything other than being sexy and interesting to boys. And the wave of sexual images, the message that my entire sense of self depended on my sex appeal, was overwhelming.
By the time I went to college, I had decided that the excitement I’d been looking for came from men and boys. If a boy wanted me, I believed that could make me worthwhile in the world—certainly every media outlet suggested that was true. And so did my father. When he commented on my friends’ bodies, I worried about my own body—was it attractive? Was I sexy like my friends? When he ogled other women on the street, he turned his eyes from me. He stopped attending to what might have also been lovable about me, such as my intelligence and sense of humor, in order to prioritize a woman’s bodily appeal. My father taught me that men care most about female’s sex appeal. He taught me that girls mattered when they served a purpose for boys.
For most of my adolescence and all of my 20’s, I used my sex appeal to try to get love and attention. I slept with lots of boys and men, many whose names I couldn’t recall if asked, many more who I thought would love me because they wanted to have sex with me. It seems naïve now, but it took me that long to understand that just because a guy wanted to have sex with me, it didn’t mean he wanted to have a relationship beyond that. It took even longer for me to understand that I could choose to have sex with a man and it didn’t mean I had to have a relationship with him.
I don’t like to blame women’s sexual and relationship issues on their fathers. It’s an outdated notion that grew from the Freudian Electra Complex. There are many other influences on a girls’ sense of sexual self, with our societal obsession with objectifying women for their bodies being the biggest. We live with many more sexual images today, more than when I was growing up. Back then there was no Internet. MTV was new, and solely showed music videos. There were all of 23 channels to surf on TV. Now that we are so inundated, though, we know more about how those images affect girls. Numerous studies have been done, books written, articles published, all informing us of the potentially negative effects.
But fathers have a responsibility to their daughters much like mothers have the responsibility to model self-love, to not put down their own or others’ bodies, and to make good choices in their relationships. Fathers can give their daughters attention for non-sexual qualities, like bravery, strength, intelligence, and humor.
Not long ago, my father told me on the telephone that he had started walking for health. I was about to let him know how pleased I was he was taking care of himself in this way when he noted that he takes the route that goes past the high school near his home so he can see the cheerleaders.
“Dad,” I said, enraged. “Those are children.”
“I’m just looking.”
“That’s disgusting,” I said.
“For God’s sake,” he said, exasperated. “You’re always so sensitive about these things.”
I am. He’s right. Because for all the times I’ve tried to explain how his behavior has affected me, he doesn’t quite get it. His enjoyment of watching young, nubile bodies dance around in short skirts is just as culturally cued as my belief that I’m made worthwhile through my sex appeal. But, I still wish he would not share such thoughts with his daughter. Perhaps had he worked to be more conscious of his own indoctrination, I could have done that work on myself too.